




With this article we will cover some of the guidelines which we like to keep in mind when writing our clinical records. This is clearly not an exhaustive list, and we encourage all health care providers to keep up to date with guidelines to ensure high standards of care, but this covers some notable ones which are captured in a consultation appointment.
1. FGDP(UK): Clinical Examination and Record-Keeping, 2016
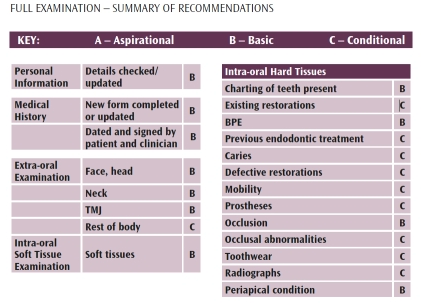
For UK based dentists, we would be remiss if this were not at the top of our list. This document provides guidance on what information should be covered in a consultation appointment, and the associated information that should be captured in the clinical notes (Paper or electronic records). Information is categorised as Aspirational (e.g. Alcohol history), Basic (e.g. Personal details being checked and updated or Medical history) and Conditional (e.g Email address) and is broken down by information captured in the dental history and clinical examination. Aspirational information is clear from the name. Basic should generally be captured unless there is a strong clinical reason why it can/should not. Conditional will not be necessary in every circumstance, but when it is, it is recommended. Different direction is provided for Full Examination, Recall and Emergency appointments. (FGDP have put together marvellous summary tables for people short of time)
2. FGDP(UK) and PHE: Guidance Notes for Dental Practitioners on the Safe Use of X-ray Equipment, 2020
This update covers a lot of employer requirements to ensure safety practice wide for employees and patients when considering dental x-rays. A key change that will affect the dentist is the quality grading system for radiographic examination. Where we previously graded 1 (Excellent), 2 (Acceptable diagnostic quality) and 3 (Unacceptable). Performance targets for this system were 70%. 20% and 10% respectively. This has been updated to A (Diagnostically acceptable) and N (Not acceptable), where targets differ for digital imaging (95% should be A, 5% N) and lm imaging (90% A, 10% N).
3. AAP/EFP New periodontal classification guidelines, 2017
The system we were using prior to this set of guidelines to diagnose periodontal disease was close to 20 years old, and included several oversights including substantial overlaps in the diagnoses and diagnostic imprecision. The new system borrows its staging and grading features from a system used to categorise disease in oncology; it creates a more accurate diagnosis of a complex disease, and therefore empowers the clinician to offer more customised treatment options based on this. The diagnostic statement should include information about area affected (Localised/Generalised/Molar incisor), the extent of current tissue loss (the stage), the rate of progression (the grade), current status (stability) and any risk factors. In Kiroku, we have this workflow built into consultation templates, linked to BPE scores of 3 or 4. It is worth noting that once a patient has been staged and graded, they will remain on the periodontal pathway in perpetuity, and this should be reflected in their diagnoses even after their periodontal health is stable.


4. BSP(UK): Guidelines for effective secondary Prevention of Periodontitis by Professional mechanical Plaque removal (PmPr),
I suppose the top line here is that in our treatment plan for perio we shouldn’t be calling them scale and polish’s anymore, they are now renamed Professional mechanical Plaque removal, PmPr for short. Root surface debridement (RSD) can now be called PmPr on root. There is a recommendation not to proceed a patient to PmPr on root unless there is evidence that they are engaged in their dental treatment, and you can see various measurements for periodontal health improving. Also included is recommendations for follow up treatment after PmPr on root, if stability is or is not achieved.

5. Delivering better oral health: an evidence-based toolkit for prevention,
Although this is likely to be known off by heart by all dental professionals, it still needs to be mentioned for it’s clear and evidence-based guidance. This set of guidelines lays out preventive advice and treatment to be provided to patients, broken down by age of the patient, from 0-3 years up to adult patients. It is a great reference for fluoride provision, whether that is recommended levels in their toothpaste, to frequency of fluoride varnish application, and acts as a good reminder to come back to ensure a high quality of care.
6. SDCEP: Prevention and management of dental caries in children, 2018
Again, within this guidance there is nothing that is likely to be new information. But it is all extremely important, and serves the dental team and their patients to review it from time to time. There are ow charts for dental pain, management of primary dentition and management of permanent dentition. All are extremely easy to digest, and act as a reminder to keep doing the things we are doing well, and perhaps add treatments we don’t do as regularly to our clinical practice. SDCEP also have brilliant apps with all their information that are easy to keep on your phone for quick access.

7. BOS: Making an orthodontic referral, 2014
Making an appropriate orthodontic referral at the right time will be profoundly impactful for a patient. Again, it is good to ensure we are fully aware of what we should be making orthodontic referrals for, and when. These guidelines cover what necessitates an early referral in the deciduous dentition or even the mixed dentition. In the
permanent dentition, it references IOTN, but reminds us that all patients have the right to a second opinion to ensure high quality patient care. It is important to keep accurate records of these decisions on when to refer.

8. AAE: Endodontic case difficulty assessment and referral
Some general dental practitioners will feel really comfortable doing more difficult endodontics, but many may not. It is really important that we are reminded of professional guidelines of when it is OK to refer on to a specialist, to ensure that the patient is receiving the best possible dental care. This set of guidelines lays out minimal, moderate and high diculty levels. With moderate and high diculty likely to result in inconsistent results even with experienced dental care practitioners. Examples of factors making the procedure more complex include position in the arch, inclination or rotation of the tooth, curvature of the roots among others. If a referral is being made, the reason should be clearly captured in the patient records.

9. NICE: Intervals between oral health reviews, 2004
These guidelines outline the shortest and longest intervals that should exist between dental check-ups, broken down by age group. They advise intervals no shorter than every three months. The longest advised period of time between appointments varies by age, no more than 12 months for the under 18s, and no more than 24 months for the over 18s. This recall interval should be done specic to each patient based on their disease risk assessment, and this should be communicated to the patient, and recorded in the patients notes.
10. FGDP(UK): Implications of COVID-19 for the safe management of general dental practice, 2020
These guidelines needed to be mentioned given the pandemic still facing the world, although they already feel woefully outdated. Broadly speaking, they breakdown the appointment to the pre-assessment, pre-treatment, treatment and after treatment. They lay out an assessment of risk, concurrent restrictions or changes we should consider to reduce the chance of infection to keep people safe, both the clinical team and the patient.
We have tried to include some of the salient flowcharts carefully put together by each body, but we must stress that the images often don’t capture the full flowchart, and certainly shouldn’t be used as replacement for reading the full guidelines. We hope though, that picking out the images here stimulates dentists to review guidelines in full they may not have seen for a little while, encouraging good patient care, high diagnostic quality and detailed records.
